

Clostridium Difficile Colitis: Causes, Symptoms & Treatment
A comprehensive, evidence-based guide to understanding C. difficile colitis — from how it develops and what symptoms to watch for, to the latest treatment strategies including antibiotics, fecal microbiota transplantation, and emerging therapies.
If you or someone you care for has recently been prescribed antibiotics and then developed persistent, watery diarrhea, the name Clostridioides difficile — commonly still referred to as Clostridium difficile or simply "C. diff" — may have come up. Understanding what it is and how it develops is foundational to informed health decisions.
C. difficile colitis is described as one of the most common healthcare-associated infections in the United States, with potential life-threatening complications and a significant burden on healthcare costs [7]. With prompt diagnosis and appropriate treatment, outcomes can be substantially improved.
✔ Quick Summary
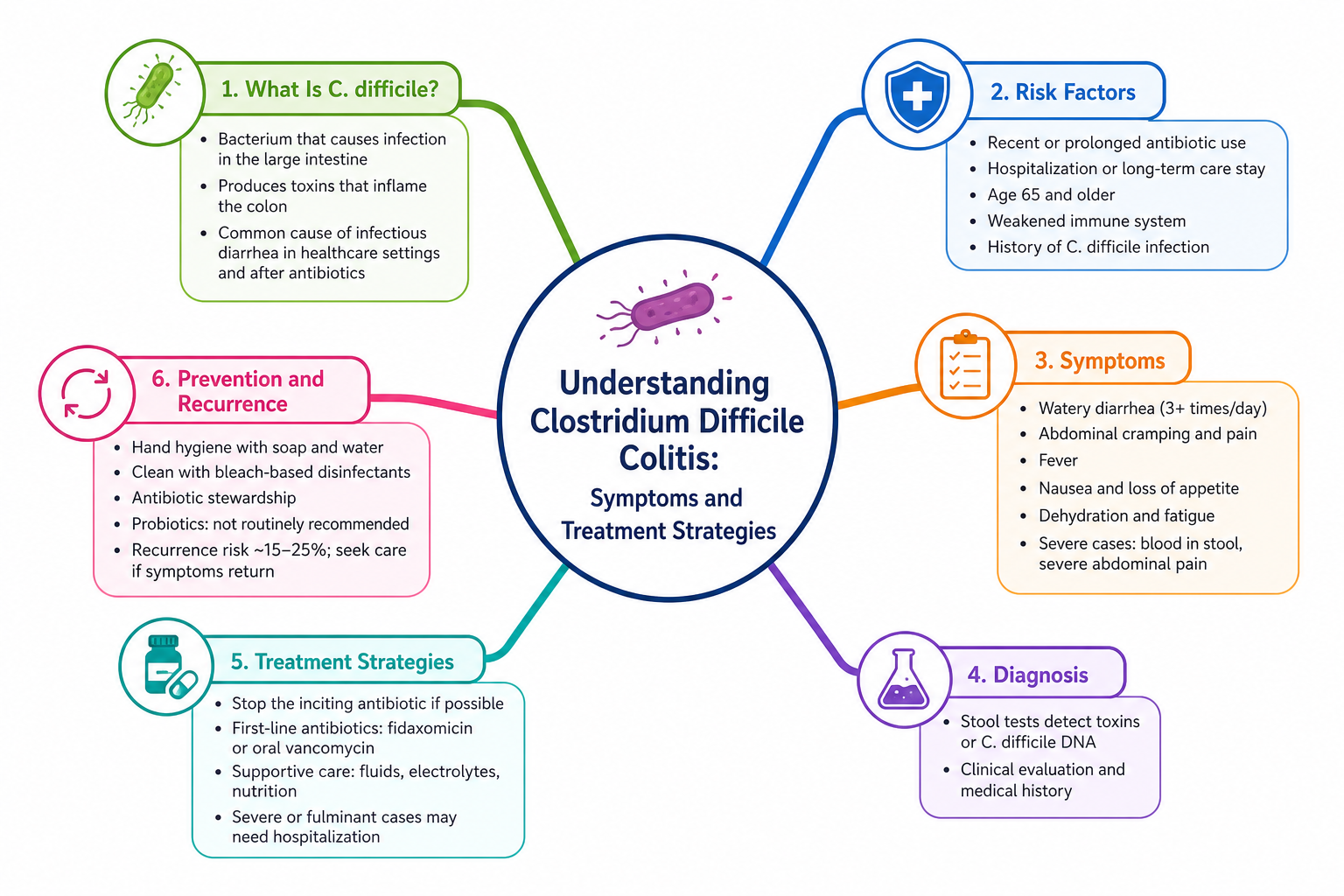
- ✓ Clostridioides difficile is a spore-forming, toxin-producing bacterium that causes colitis primarily after antibiotic use disrupts the gut microbiome [6].
- ✓ Clinical presentation ranges from mild diarrhea to severe, life-threatening colitis; prompt diagnosis is essential [6][9].
- ✓ First-line treatments include vancomycin and fidaxomicin; metronidazole is considered an inferior option [6][7].
- ✓ Fecal microbiota transplantation (FMT) is effective for recurrent infection and has been shown to restore a healthy bile acid composition in the gut faster than vancomycin or bacterial mixtures [1][7].
1. What Is Clostridium Difficile Colitis?
Clostridioides difficile (formerly classified as Clostridium difficile) is a Gram-positive, spore-forming, anaerobic bacterium — meaning it thrives in environments with little to no oxygen [6]. It is widely distributed in the intestinal tracts of humans and animals, and in the surrounding environment, including hospital surfaces and soil [6][9]. When conditions in the gut become disrupted — most often following antibiotic use — this organism can multiply and produce powerful toxins that damage the inner lining of the colon, leading to C. difficile infection (CDI) and colitis.
In the last decade, the frequency and severity of CDI has been increasing worldwide, making it one of the most common hospital-acquired infections globally [6]. While it has long been recognized in North America and Europe, CDI is increasingly emerging in Asia as well [9].
Clostridioides difficile infection is described as the most common healthcare-associated infection in the United States, with potential life-threatening complications and significant impact on healthcare costs [7]. Its spores are resistant to many standard cleaning agents, making control of hospital transmission particularly challenging [6].
2. How Does Clostridium Difficile Colitis Develop?
The gut microbiome normally functions as a balanced ecosystem in which diverse bacterial communities inhibit the growth of pathogenic organisms. Antibiotics, while essential therapies, can disrupt this ecosystem broadly, eliminating populations of beneficial bacteria and creating conditions that C. difficile is well positioned to exploit [8].
Once normal gut flora is disrupted, C. difficile spores — transmitted via the fecal-oral route through contaminated hands, surfaces, or food — can germinate and colonize the colon [6]. Research has shown that patients with CDI have elevated colonic levels of primary bile acids, which act as potent stimulators of C. difficile spore germination [1]. Under healthy conditions, commensal gut bacteria convert primary bile acids into secondary bile acids that inhibit C. difficile growth. When this conversion is disrupted by dysbiosis, C. difficile gains a significant survival advantage [1][8]. Laboratory research has confirmed that ulcerative colitis microbiotas are innately susceptible to C. difficile colonization, while healthy microbiotas resist it — consistent with clinical observations [2].
Once established, C. difficile produces two key toxins: Toxin A (TcdA) and Toxin B (TcdB). TcdB has been shown in experimental models to inhibit its internalization into host cells, disrupt self-cleavage mechanisms, and interfere with Rac1 glycosylation, causing widespread epithelial damage and colonic inflammation [5]. The clinical result ranges from watery diarrhea to severe, life-threatening colitis.
⚠️ Who Is Most at Risk?
While CDI can affect anyone, certain groups face a substantially elevated risk. The three most important classical risk factors are antibiotic therapy, advanced age, and hospital or nursing home residence [6], but several other contributors are clinically relevant.
Recent Antibiotic Use: The single most important risk factor. Broad-spectrum antibiotics disrupt the protective gut microbiome, creating conditions in which C. difficile can proliferate and produce toxins [6][8].
Advanced Age: Older adults have reduced immune function and altered gut microbial composition, increasing susceptibility to CDI and its complications [6][9].
Hospitalization or Nursing Home Residence: Healthcare settings harbor C. difficile spores on surfaces and equipment, increasing the probability of exposure [6][9].
Inflammatory Bowel Disease (IBD): Patients with Crohn’s disease or ulcerative colitis face an increased risk of symptomatic CDI, attributable to underlying gut dysbiosis, immune dysregulation, and immunosuppressive therapies [10]. Laboratory evidence confirms UC microbiotas are innately susceptible to C. difficile colonization while healthy microbiotas show resistance [2].
Chronic Acid-Suppressive Therapy: Antibiotic stewardship combined with discontinuation of unnecessary acid suppression is considered key for CDI prevention and treatment [7].
Delayed Surgical Procedures or Ileostomy Reversal: A retrospective cohort study of 223 patients found that delayed loop ileostomy reversal — particularly beyond approximately 134 days — is statistically associated with increased risk of post-operative colitis and C. difficile infection (OR 1.11, p = 0.020) [4].
Immunosuppression: Patients on corticosteroids or other immunosuppressive agents have a reduced ability to clear C. difficile. In IBD patients specifically, corticosteroid use and unnecessary broad-spectrum antibiotics are identified as modifiable risk factors for severe CDI [10].
3. Signs & Symptoms
The clinical picture of CDI is diverse — ranging from an entirely asymptomatic carrier state to severe, life-threatening colitis [6]. The following are the recognized clinical features:
Watery Diarrhea: The hallmark symptom. TcdA and TcdB damage the colonic epithelium, impairing water and electrolyte absorption and producing frequent, loose, often foul-smelling stools [6][8].
Abdominal Cramping and Pain: Colonic inflammation triggers painful muscle contractions ranging from mild discomfort to severe, debilitating pain [6][9].
Fever: Systemic inflammation in response to toxin-mediated colonic injury commonly produces elevated body temperature, which may signal worsening disease [6].
Nausea and Loss of Appetite: Colonic inflammation and gut dysmotility can suppress appetite and cause nausea, contributing to nutritional depletion in prolonged cases [9].
Blood or Mucus in Stool: In more severe forms, mucosal damage can result in blood or mucus in stool — a sign warranting urgent evaluation [6].
Dehydration and Electrolyte Imbalance: Profuse diarrhea depletes fluids and electrolytes, potentially causing weakness, dizziness, and acute kidney injury, also observed as a post-operative complication in surgical patients with CDI [4].
Toxic Megacolon or Colonic Ileus (Severe Cases): In the most serious presentations, the colon can dilate dangerously (toxic megacolon) or cease normal movement (ileus), representing surgical emergencies [6][9].
Asymptomatic Carrier State: Some individuals harbor C. difficile without developing symptoms. This carrier state poses a transmission risk in healthcare settings and may transition to active disease if additional risk factors emerge [6].
4. How Is Clostridium Difficile Colitis Diagnosed?
🔬 Differential Diagnosis & Investigations
Diagnosing CDI requires both clinical suspicion and appropriate laboratory testing. Diarrhea in a patient who has recently received antibiotics or is in a healthcare setting should prompt immediate testing. No single laboratory test is sufficient as a stand-alone confirmation of CDI, and a two-step diagnostic approach is generally recommended [6][7]. Clinicians must also rule out other conditions that can mimic CDI, including IBD flares, other infectious colitides, and — in immunocompromised or at-risk patients — parasitic infections [3].
Diagnosis is based on direct detection of C. difficile toxins in feces, most commonly using enzyme immunoassay (EIA). No single test is reliable as a stand-alone confirmation [6]. Current best practice favors a two-step diagnostic approach — typically combining a highly sensitive screening test (such as a glutamate dehydrogenase antigen test or nucleic acid amplification test) with a confirmatory toxin assay — to improve both sensitivity and specificity [7]. In recurrent or complex cases, techniques such as 16S rDNA gene sequencing have been used in research settings to characterize the gut microbial environment and identify bile acid-metabolizing bacteria relevant to treatment response [1].
5. Treatment Options
Effective management of CDI depends on disease severity, whether the episode is an initial or recurrent infection, and the patient’s underlying health status. Antibiotic stewardship — stopping unnecessary antibiotics and discontinuing chronic acid-suppressive therapy when not indicated — forms the cornerstone of both prevention and treatment [7].
🏢 A. First-Line Treatment
Vancomycin and fidaxomicin are the established first-line antibiotics for CDI; metronidazole is considered an inferior option and is generally no longer recommended as primary therapy [6][7]. Vancomycin is administered orally and acts locally within the colon. Fidaxomicin, a macrocyclic antibiotic, has a more targeted spectrum of activity that spares more of the commensal microbiota compared to broad-spectrum agents [7]. Stopping the precipitating antibiotic when clinically possible is a critical parallel intervention [7]. In surgical patients, ensuring timely ileostomy reversal within recommended timeframes may reduce CDI risk [4].
💊 B. Management of Recurrent CDI
- Vancomycin (oral): Used for initial and recurrent episodes. A randomized controlled trial subgroup analysis showed that vancomycin treatment shifts bile acid composition toward secondary bile acid dominance, though this occurs more slowly than with FMT [1][6].
- Fidaxomicin: A preferred option for recurrent CDI due to its narrow-spectrum activity and relative sparing of commensal gut flora [7].
- Bezlotoxumab: A monoclonal antibody targeting C. difficile toxin B (TcdB), proven effective in reducing recurrent CDI. It addresses the toxin-mediated disease mechanism without acting as an antibiotic, thereby avoiding further microbiome disruption [7][10].
- Fecal Microbiota Transplantation (FMT): Established as an effective strategy for recurrent CDI, with a robust profile of safety and effectiveness in adults and children [7][10]. A randomized controlled trial subgroup analysis demonstrated that FMT restores a donor-like dominance of secondary bile acids — which inhibit C. difficile germination — significantly faster than vancomycin alone or a 12-strain bacterial mixture, reducing the window of susceptibility to recurrence [1].
- Live Biotherapeutic Products (Bacterial Mixtures): Emerging alternatives to donor stool for treating recurrent CDI. Current evidence suggests these products may benefit from the inclusion of bile acid-metabolizing bacteria, as their restoration of secondary bile acid dominance occurs later than with FMT [1][7].
- Antivirulence Compounds (Experimental): In preclinical models, compounds including myricetin and its derivatives have been shown to suppress TcdB-mediated cellular damage, promote beneficial bacteria (including Muribaculaceae and Lactobacillaceae), and elevate protective metabolites such as indole derivatives [5]. These approaches have not yet been evaluated in human clinical trials.
🏠 C. Supportive Management
Supportive care is essential alongside antibiotic therapy. Oral or intravenous rehydration is required to replace fluids and electrolytes lost through diarrhea. Nutritional support should be provided as tolerated. Patients should practice hand hygiene with soap and water — alcohol-based hand rubs are less effective against C. difficile spores — and inform all healthcare providers of their CDI history to guide future antibiotic decisions [6][9]. In IBD patients, modifiable risk factors including ongoing corticosteroid use and unnecessary broad-spectrum antibiotic exposure should be minimized [10]. For hospitalized patients, contact precautions and environmental decontamination are essential to prevent spread [6].
📚 Evidence in Context
Vancomycin and fidaxomicin are well-supported as first-line agents, with metronidazole now considered inferior [6][7]. FMT is robustly supported for recurrent CDI, with randomized controlled trial subgroup data specifically demonstrating its superiority in restoring bile acid homeostasis compared with vancomycin or a 12-strain bacterial mixture — providing a mechanistic basis for its efficacy in preventing recurrence [1]. Bezlotoxumab and live biotherapeutic products represent validated novel options addressing microbiome restoration [7][10]. Important uncertainties remain: the optimal bacterial composition of FMT alternatives is still being defined, and the inclusion of bile acid-metabolizing bacteria in these products may be critical [1]. Antivirulence strategies such as myricetin derivatives show promise in animal models but have not yet been evaluated in human clinical trials [5]. In patients with IBD, CDI masquerading as a disease flare remains a significant diagnostic challenge requiring a high index of suspicion and prompt testing [10]. In immunocompromised patients from endemic regions, rare but fatal conditions such as disseminated strongyloidiasis can mimic CDI and IBD, underscoring the importance of parasitological screening before immunosuppressive therapy [3]. Individual patient factors — recurrence risk, immune status, and comorbidities — must always guide clinical decision-making.
6. When to Seek Emergency Medical Help
• You develop severe or rapidly worsening abdominal pain that is disproportionate to prior symptoms.
• Diarrhea is bloody or contains significant mucus and is associated with fever.
• You experience signs of dehydration: extreme thirst, markedly reduced urination, dizziness, or confusion.
• You develop a distended, rigid abdomen — which may indicate toxic megacolon or colonic ileus, both surgical emergencies [6][9].
• You have a known diagnosis of CDI and your symptoms suddenly worsen despite treatment, or you develop a high fever and systemic deterioration.
• You are immunocompromised (e.g., on corticosteroids or biologics) and develop new or worsening colitis symptoms — including if CDI testing returns negative, as other serious conditions such as disseminated strongyloidiasis must be excluded [3][10].
7. Frequently Asked Questions
References
- Subgroup analysis from FMT randomized controlled trials. *Bile acid composition and bacterial dynamics in CDI.*
- In vitro model analysis of UC microbiota susceptibility. *Gastroenterology Research.*
- Case report: Unrecognized strongyloidiasis mimicking IBD/CDI. *Journal of Clinical Parasitology.*
- Retrospective cohort study on loop ileostomy reversal delay. *Surgical Endoscopy.*
- Preclinical models of TcdB-mediated cellular damage and antivirulence compounds. *Microbiome and Pharmacology.*
- Clinical practice guidelines for Clostridioides difficile infection. *Infectious Diseases Society of America (IDSA).*
- Antibiotic stewardship and FMT guidelines. *American College of Gastroenterology (ACG).*
- Role of gut microbiome disruption in antibiotic-associated diarrhea. *Nature Reviews Gastroenterology.*
- Global epidemiology of C. difficile infections. *World Journal of Gastroenterology.*
- Management of C. difficile in Inflammatory Bowel Disease. *Gastroenterology & Hepatology.*